Key Takeaways
- Most hospitals can’t act on data fast enough to support timely decisions.
- Real-time failure leads to clinical risk, AI breakdowns, and operational drag.
- 64% of hospitals lack real-time readiness across core systems.
- Fixing it requires governance, streaming-first architecture, and MLOps.
- Enterprise AI plays a dual role: consuming and harmonizing real-time data.
- Hospitals that invest in real-time infrastructure improve outcomes and gain agility.
Ask five health systems what “real-time” means, and you’ll get five different answers.
In the ICU, real-time means milliseconds. Every heartbeat, every oxygen dip, every spike in blood pressure—streamed continuously, not cached or delayed.
But in most hospital environments, the definition gets softer. A lab result every few hours. A vitals update on the hour.
In outpatient care? Sometimes it’s end-of-day batching, and that’s still called “real-time.”
That’s the problem.
The Reality Check
According to recent data, 64% of hospitals lack the infrastructure to operate on real-time data across their core systems. It’s not a software issue, it’s systemic. Most data arrives too late, too noisy, or too fragmented to act on.
And that delay has a cost.
Why It Matters Now
Enterprise AI doesn’t run on stale data. Neither does clinical decision support. And as health systems stretch to manage volumes, acuity, and resource constraints, the ability to move with the moment is no longer optional.
Without real-time data flow:
- Predictive AI breaks down before it starts
- Care coordination slows under outdated context
- Operational agility disappears—ORs back up, staffing misfires, discharges stall
Hospitals talk about precision care. But if data can’t move when and where it’s needed, precision stays theoretical.
Six Root Causes Behind the Real-Time Breakdown
If real-time data is so essential, why do so few hospitals have it?
Because the gap is structural, not as much technical. Most health systems weren’t built for speed, scale, or system-wide visibility.
The result: a stack of underlying issues that make real-time data feel impossible.
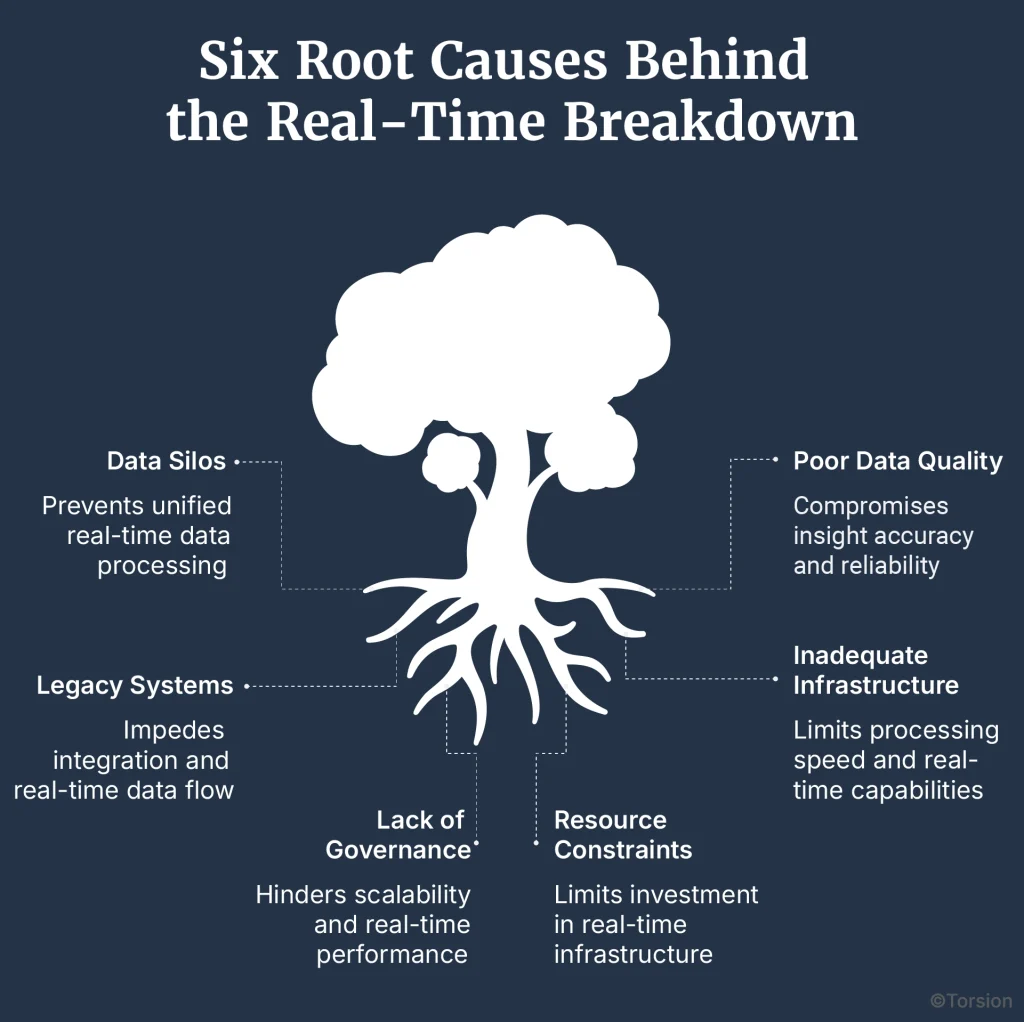
1. Data Silos That Refuse to Talk
Systems don’t fail to talk because they’re broken. They fail to talk because they were never meant to.
Radiology, lab, pharmacy, billing each built with its own logic, models, and language. EHRs often sit at the center, but they don’t unify. They warehouse.
Impact:
- Redundant charting
- Missed context at the point of care
- No longitudinal patient view
Technical friction:
- Proprietary APIs
- Inconsistent data models
- No shared schema translation layer
2. Garbage In, No Insight Out
Fast data isn’t the same as good data.
Real-time streams are often incomplete, misaligned, or delayed just enough to be useless. Some lack proper timestamps. Others get buried in manual workflows before they’re even usable.
Impact:
- Broken CDS logic
- Faulty model training
- Rising clinician distrust
What’s missing:
- Real-time schema validation
- Event-level audit trails
- Timestamp integrity
3. Legacy Systems and the Interoperability Wall
Most hospitals still run on infrastructure that predates the modern web. And when these systems can’t evolve, they isolate.
Impact:
- Vendor lock-in
- Technical debt that compounds annually
- High-friction integrations
Root causes:
- No FHIR support
- Static data exchanges (batch uploads, CSV dumps)
- No support for event-driven architecture
4. Infrastructure Not Built for Velocity
Real-time data is about how you move, store, and query at scale, along with software.
Impact:
- Bottlenecks in high-acuity environments
- Missed packets from ICU monitors or wearables
- Laggy dashboards that undercut decision-making
Stack gaps:
- No Kafka or Flink adoption
- Data lakes that don’t support live updates
- No edge ingestion at the bedside
5. No Governance = No Scalability
You can’t scale what no one owns. And in many systems, real-time data lacks clear ownership.
Impact:
- Compliance gaps
- Privacy risks
- Fragmented data flows across teams
What’s absent:
- Stream metadata standards
- Real-time audit logs
- Lifecycle policies for live data
6. Cost and Capability Constraints
Even for systems that want to fix this, talent and budget are real constraints.
Impact:
- Mid-size hospitals stuck with vendor lock-in
- No internal muscle to scale past the PoC
- High ongoing costs to maintain even basic reliability
Skill shortages:
- Stream engineers
- Real-time MLOps leads
- Architects who understand failover at scale
The Ripple Effects: When Real-Time Becomes Real Risk
Hospitals don’t fall behind because they lack data. They fall behind because they can’t move it fast enough, or trust it when it arrives.
When real-time readiness breaks down, the consequences ripple across every layer of care delivery. And unlike technical debt, these impacts show up in clinical outcomes, staffing models, and strategy decks.
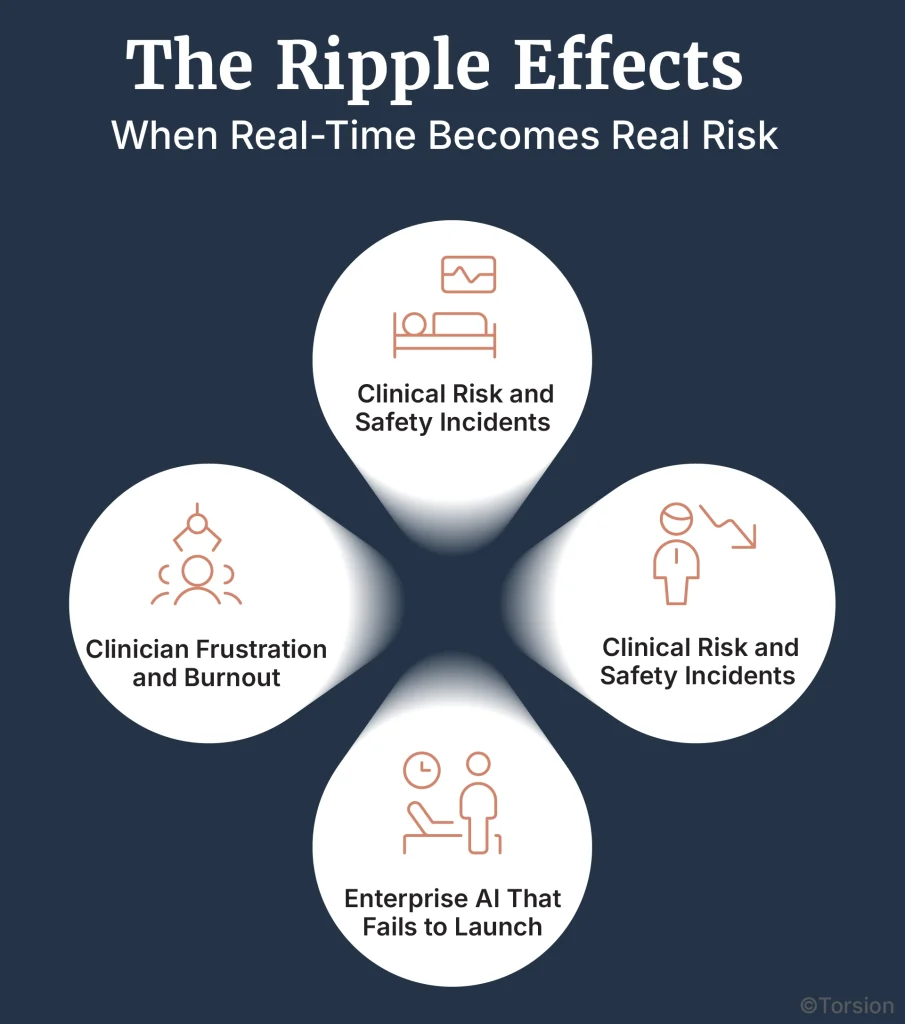
A. Clinical Risk and Safety Incidents
When data is late or missing, decisions happen in the dark.
Delayed deterioration alerts. Incomplete vitals during triage. Misdiagnoses because a key lab result was buried in a system that didn’t sync fast enough.
Real-time failure isn’t hypothetical. It’s what happens when a nurse documents an event after it matters. Or when a CDS tool fires off the wrong alert because it missed a timestamp shift.
Studies have linked data latency and alarm fatigue to increased diagnostic delays and adverse patient outcomes, particularly in critical care and high-acuity settings.
B. Operational Inefficiency and Hidden Costs
Hospitals with stale data lose time in every direction:
- Patient flow slows down because discharges aren’t triggered
- OR utilization dips because schedules rely on outdated census data
- Staffing misfires because there’s no real view of acuity or shift demand
These inefficiencies don’t show up as line items, but they’re real. Some systems report that real-time analytics can cut patient wait times by up to 30% and improve staff satisfaction in the process.
C. Enterprise AI That Fails to Launch
Most Enterprise AI projects fail because the inputs are stale, rather than the model being wrong.
In one survey, 42% of organizations reported Enterprise AI failures tied to data readiness. And when you can’t stream fresh, reliable signals into your CDS or prediction tools, real-time Enterprise AI stops being real and starts being another stalled investment.
Even simple alerting becomes impossible when models operate off data that’s already out of date.
D. Clinician Frustration and Burnout
Doctors and nurses don’t want more data. They want the right data, at the right time.
When systems fail to surface what matters, clinicians resort to manual workarounds. Hunting across systems. Rechecking lab results. Documenting twice to cover gaps. Over time, this erodes trust and adds to digital fatigue, already a top contributor to clinician burnout.
EHR bloat and broken data flows are among the most commonly cited stressors in provider surveys.
The Blueprint for Real-Time Readiness: An Enterprise AI Approach
Fixing the real-time deficit doesn’t start with an algorithm. It starts with the foundation.
You don’t need to rip and replace your entire tech stack. But you do need to rethink how systems talk, how data moves, and how teams are aligned around it. The goal isn’t speed for the sake of speed, it’s to surface insight that’s accurate, timely, and trusted.
Here’s what that takes.
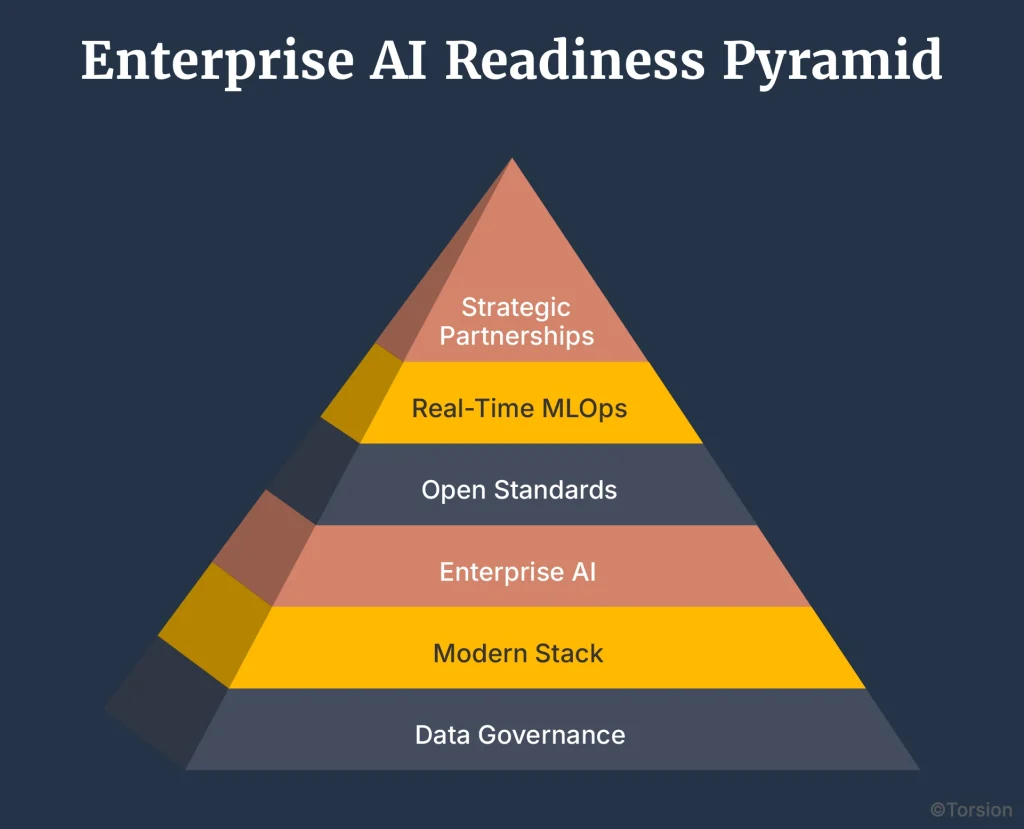
A. Start With Data Governance and Quality at the Core
Before you build anything real-time, you have to fix what’s upstream.
- Standardize how data enters the system from bedside devices to manual entries.
- Validate data at the source, not after the fact.
- Assign ownership to the real-time data lifecycle, with event-level auditing and access controls.
The pandemic made it clear: without clear governance, even good data becomes a liability. Rebuilding trust starts here.
B. Modernize the Stack: Architect for Streaming First
Batch pipelines can’t support real-time care.
- Adopt tools like Apache Kafka, Spark Streaming, or Apache Flink for continuous ingestion.
- Shift toward lakehouse architectures (e.g., Delta Lake, Iceberg) that combine the scalability of data lakes with the structure of warehouses.
- Push data capture to the edge ICUs, telemetry units, remote monitoring nodes—so insights don’t rely on delayed central syncs.
C. Use Enterprise AI to Harmonize and Connect
Real-time isn’t helpful if the data is disjointed.
- Use NLP to extract meaning from clinical notes in motion
- Deploy AI-based entity resolution to unify patient records scattered across departments
- Automate schema and terminology matching across vocabularies like SNOMED CT, ICD-10, and LOINC
This is where Enterprise AI plays offense, not just consuming data, but making it usable across systems.
D. Embrace Open Standards and an API-First Culture
Interoperability is capability and compliance combined.
- Lead with FHIR-first architecture for every new system or data exchange
- Secure every stream with OAuth2, RBAC, and token-based access
- Build internal API marketplaces so teams can discover, integrate, and share data services faster
Systems that share well move faster, recover faster, and scale better. This is the long game.
E. Operationalize With Real-Time MLOps
Real-time Enterprise AI needs real-time upkeep.
- Monitor model health on live streams, not just on test data
- Retrain based on data drift, not quarterly reviews
- Create fail-safes for alert fatigue, false positives, and performance dips under pressure
With 42% of Enterprise AI projects stalling due to data issues, real-time MLOps is has become a requirement.
F. Partner Where It Counts
Not every team can build this from scratch and that’s okay.
- Bring in specialists to design stream-first architecture or embed real-time MLOps practices
- Focus on measurable ROI: reduced latency, faster handoffs, improved patient throughput
- Avoid vendor lock-in by choosing partners who teach as they build
The point isn’t to outsource. It’s to accelerate your internal muscle so transformation doesn’t die at the pilot stage.
From Static to Streamed: Rewiring the Future of Patient Data
Most hospitals aren’t missing data, they’re stuck with data that doesn’t move.
After decades of digitization, the problem is relevance. Information arrives too late, too fragmented, or too unreliable to support the decisions that matter most.
That’s the real-time deficit.
Real-Time Is About Timing, Not Speed.
When vitals from an ICU monitor don’t sync fast enough, it’s a clinical risk instead of a latency issue. When Enterprise AI predictions run on stale lab values, that’s a patient safety problem. And when CDS tools fire on incomplete context, trust erodes at the frontline.
Hospitals can’t afford to treat real-time as an IT upgrade. It’s a system-wide imperative.
The Data Is There. Now It Needs to Move.
The tech exists. The standards exist. Even the incentives are starting to align. What’s needed now is leadership that treats real-time data as a strategic asset.
Hospitals that get this right will:
- Cut operational drag
- Boost Enterprise AI reliability
- Reduce clinician fatigue
- And deliver faster, safer care across every unit